



Getting pregnant with Hashimoto’s © fertility-tv.com
Getting pregnant with Hashimoto’s – is it possible? I use my experience and studies to show you how you can fulfill your desire to have children.
Getting pregnant is a central goal in life for many couples. But if a woman suffers from Hashimoto’s thyroiditis, this can lead to uncertainty. Hashimoto’s thyroiditis is an autoimmune disease in which the immune system attacks the thyroid gland, leading to chronic inflammation. This inflammation can affect the production of thyroid hormones, which is important for regulating the menstrual cycle, ovulation and fertility. I myself know how difficult it is to get pregnant with Hashimoto’s. After all, I’ve tried and succeeded twice, so I’m sharing my experiences in this post.
What is Hashimoto?
Hashimoto’s thyroiditis is an autoimmune thyroid disease in which the immune system mistakenly attacks the thyroid gland, leading to chronic inflammation. This can damage the thyroid gland and impair its ability to produce hormones, often leading to hypothyroidism (underactive thyroid). Symptoms can include fatigue, weight gain, sensitivity to cold, hair loss and mood swings.
Does Hashimoto’s disease affect fertility?
Hashimoto’s thyroiditis, a form of autoimmune thyroiditis, can have an impact on fertility, especially in women. The disease leads to hypothyroidism, a condition in which the thyroid gland does not produce enough hormones. Thyroid hormones play an important role in the regulation of the menstrual cycle, ovulation and general reproductive health.
Longer menstrual cycles and lack of ovulation
Studies have found evidence that hypothyroidism, as can occur with Hashimoto’s, is associated with fertility problems, including longer menstrual cycles, anovulation (lack of ovulation) and increased miscarriage rates. A study by Arojoki et al (2000) found that antibodies to thyroid peroxidase (TPO antibodies), an indicator of Hashimoto’s thyroiditis, were more common in infertile women. In the study of over 350 women who wanted to become pregnant with Hashimoto’s, over 30% of women with Hashimoto’s had a prolonged cycle.
Increased risk of miscarriage
A survey study examined women who wanted to become pregnant with Hashimoto’s and used ICSI or IVF as a means of achieving this. The results showed that the autoimmune thyroid disease had no influence on the ICSI or IVF pregnancy rate. However, the study found an increased miscarriage rate and reduced live birth rate in women with Hashimoto’s compared to the control group. In further studies by Poppe and Velkeniers, the first hormonal causes for the connection between Hashimoto’s and the increased miscarriage rate were discovered.
Reduction of the miscarriage rate through thyroid hormones
Treatment with thyroid hormones may be necessary for women who have Hashimoto’s thyroiditis and have difficulty getting pregnant. Such treatment can improve fertility rates and reduce the risk of recurrent miscarriage. For example, a study by Negro et al (2006) demonstrated the effectiveness of thyroid hormone therapy in reducing miscarriage rates and other complications in pregnant women with TPO antibodies.
In summary, uncontrolled Hashimoto’s thyroiditis can pose a risk of fertility problems. However, with appropriate treatment, the balance of thyroid function can be restored, which in turn can increase the chances of successful conception and pregnancy.
Which symptoms are more common with Hashimoto’s?
Hashimoto’s thyroiditis often leads to a range of symptoms that begin gradually and can worsen over time. The variety of symptoms is caused by reduced hormone production by the thyroid gland. The most common signs include:
Persistent exhaustion
Many sufferers feel constantly tired, even if they get enough sleep.
Unexplained increase in body weight
People can experience weight gain even if they have not changed their diet.
Sensitivity to cold
Those affected often freeze easily, even in situations that others perceive as warm.
Skin and hair changes
The skin can become dry and brittle. Hair loss and brittle nails are also not uncommon.
Digestive problems
A slow metabolism can lead to regular constipation.
Voice changes and swollen tongue
The voice may seem hoarse and the tongue may feel swollen, especially if there is swelling of the thyroid gland.
Menstrual cramps
In women, menstrual cycles can be more irregular or more intense.
Muscle and joint complaints
Stiffness, pain and weakness in muscles and joints are not uncommon.
Psychological stress
Depression or reduced cognitive functions such as memory problems can occur more frequently.
Goitre formation
A visible swelling in the neck area, known as a goitre, can develop in some people.
If such symptoms occur, a medical examination is advisable. Tests to determine hormone levels and antibodies against thyroid tissue help to make a diagnosis. Sometimes an ultrasound examination of the thyroid gland is also carried out. Personally, I mainly had to deal with dry skin, sensitivity to cold, goitre formation as well as persistent exhaustion and tiredness, which is why I went to the doctor as a teenager.
How is Hashimoto’s diagnosed?
The typical procedure for Hashimoto’s diagnosis is actually always similar.
Preliminary consultation and symptom assessment
The attending physician will first of all record the symptoms in a preliminary consultation and see whether they fit in with the symptoms of thyroid disease.
Blood tests
This is followed by special blood tests that indicate an underactive thyroid. Here, for example, TSH is elevated and the low free thyroxines (T3 and T4) are usually reduced. Furthermore, a test for antibodies against the thyroid enzyme thyroperoxidase can confirm the suspicion of an autoimmune disease.
Ultrasound examination of the thyroid gland
Finally, an ultrasound examination of the thyroid gland is often carried out, as in my case, where tissue changes and inflammation of the thyroid gland can be detected. The size of the thyroid gland is also an indication of an autoimmune disease.
How is Hashimoto’s typically treated?
The treatment of Hashimoto’s thyroiditis is mainly based on symptoms and blood values. Doctors often prescribe lifelong thyroid hormones (usually levothyroxine) to compensate for a hormone deficiency and alleviate the symptoms of hypothyroidism. The dosage is adjusted individually and regularly checked by blood tests to keep the levels in the optimum range. A healthy diet and regular check-ups can help to control thyroid disease. I personally followed this therapy for many years and in the end chose a natural treatment against the doctors’ advice.
Getting pregnant with Hashimoto’s my experiences
I personally got pregnant twice with Hashimoto’s and now I’m sharing what I did to get pregnant.
Getting pregnant with Hashimoto’s with L-thyroxine
During my first pregnancy, I simply ate a “normal mixed diet” and took L-thyroxine. At 26, I was also at a good age to get pregnant. I also used the Symptothermal method to determine my ovulation and fertile days.
Getting Pregnant with Hashimotos Experience without L-Thyroxin © fertility-tv.com
Start of my period
My cycle started with my period on January 18, 2012 and ended on October 31, 2012 with the birth of my second desired child.
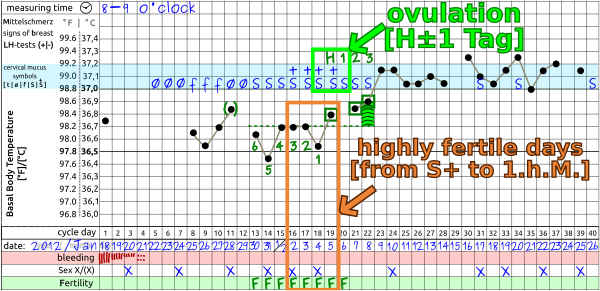
Ovulation and fertilization
NFP definitely makes it easier to get pregnant with Hashimoto’s. I simply took my temperature every morning and monitored my cervical mucus. I entered the mucus quality (Ø, f,S,S+) together with the measured body temperature in a cycle sheet. I evaluated the resulting temperature curve and the course of the mucus according to the NFP rules and was able to determine ovulation with 91% certainty in the period from February 3 to 6, 2012. On February 4, 2012, I had unprotected sex, which probably led to pregnancy.
Pregnancy determined by temperature curve
If you are pregnant with Hashimoto’s, your basal body temperature will remain elevated for at least the first trimester of pregnancy. Your period is also usually absent. Therefore, according to the NFP rules, I was able to recognize my pregnancy on 22 February 2012 from the temperature curve because my temperature did not drop for 18 days and my period did not come.
Getting pregnant with Hashimoto’s without L-thyroxine
During my second pregnancy, I dared to try a bold experiment and stopped taking the thyroid hormone L-thyroxine around 9 to 12 months before my pregnancy due to severe side effects such as severe hot flushes, cardiac arrhythmia, etc. My doctor warned me of the risks, but I wanted to take a different approach. Of course, my doctor pointed out the risks to me, but I wanted to take a different approach. My TSH was 7 mU per liter, well above the normal range of 0.5 – 4.6 mU per liter. My cycles showed a prolonged egg maturation phase and a shortened corpus luteum phase.
Naturopathic treatment
I treated my thyroid gland holistically with special thyroid globules Thyreoidea and took two globules a day about 30 minutes before eating in the morning, at lunchtime and in the evening. I also took special T3 and T4 globules from the online market pharmacy. I also received a vitamin B12 injection and supplemented vitamin D3 with K2, magnesium and took selenium via Brazil nuts (2-3 pieces) per day.
Acupuncture and thyroid yoga
Before the treatment, my luteal phase was significantly shortened and almost always just under 10 days long. This was clearly too short for successful implantation of the egg. I finally went to a TCM practice. At this time, I started a cure with homemade root vegetable broth and drank it daily – this was a recommendation from my TCM therapist. After a few appointments with the TCM therapist and acupuncture, my luteal phase suddenly extended to 11 days. This meant that I was able to get pregnant naturally, at least in terms of my cycle. I also practiced thyroid yoga to strengthen my thyroid gland in a holistic and natural way.
Liver cleanse and intestinal detox
During this period, I also carried out a liver cleanse and intestinal detox following instructions from a nutrition expert, which was also intended to give my body a boost.
Gluten-free diet based on the autoimmune protocol
At that time, I was eating a vegetarian or almost completely vegan diet and predominantly gluten-free according to the autoimmune protocol and tried to avoid processed products for the most part.
TSH value improvement
All the measures eventually led to my TSH level dropping from 7 mU per liter to around 2 to 4 mU per liter, which was within the normal range. The whole process took about 6 to 9 months until my body was ready to get pregnant with Hashimoto’s again.
Getting Pregnant with Hashimotos without medication © fertility-tv.com
Period and cycle
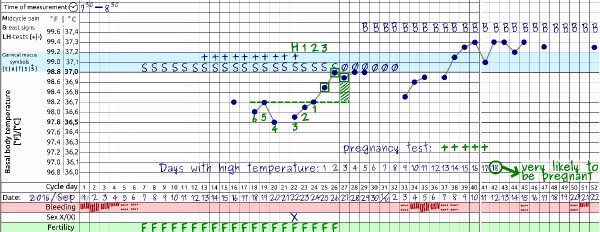
My second pregnancy cycle began on September 1, 2016 and ended on June 24, 2017 with the birth of my second dream child.
Ovulation and fertilization
As already described, I was able to determine my ovulation with NFP using the temperature curve in the period from September 23 to 26, 2016. On 22 September 2016, I only had unprotected sex once in this cycle, which clearly led to fertilization. Therefore, September 22, 2016 was also the day of conception.
Heavy implantation bleeding during my period
During this cycle, I had heavy implantation bleeding between October 4 and 6, 2016 as a sign of pregnancy. This is a rare phenomenon, but it can occur if part of the mucous membrane detaches and bleeds during implantation of the egg in the uterine lining.
Positive Pregnancy test
On October 7, 2016, I successfully tested for pregnancy with the Clearblue pregnancy test. The pregnancy was later confirmed at the birth center via a blood test. Overall, I was doing very well during my pregnancy and gave birth to my child in a healthy home birth in a bungalow and documented it on YouTube.
Fazit
Yes, its getting pregnant with Hashimoto’s is possible. However, this requires a good team of naturopaths and doctors and the right attitude. If you decide to take the classic route with medication, the thyroid values TSH, T3 and T4 as well as the abnormalities of the thyroid gland must be checked regularly. Too high a TSH value is linked to low birth weight, premature birth and much more. Chronic diseases such as diabetes are also more common in children born to women with Hashimoto’s.
Everybody is the architect of his own destiny
The Roman politician Appius Claudius Caecus coined the popular saying: “Everybody is the architect of his own destiny”. Due to the severe side effects of thyroid medication, I made a medically risky decision to treat an officially incurable disease naturally. The book by Dr. Bernd Rieger *”Hashimoto and Basedow: treating and curing thyroid disease holistically” gave me strength and courage. I would also like to thank my doctor and alternative practitioner, who provided me with excellent support along the way. Every woman has to take the risk of such a decision herself, but it worked for me and I now live without medication and feel healthy. I have two healthy children and am happy with the way everything turned out.
But regardless of whether you get pregnant naturally with Hashimoto’s or the traditional way, I wish you all the best on your way to your dream child.
Please note
This article is for information purposes only and does not constitute medical advice. Please always consult a doctor or pharmacist you trust if you have any questions about risks, side effects or appropriate treatment.
Sources
[1] Arojoki M, Jokimaa V, Juuti A, Koskinen P, Irjala K, Anttila L. Hypothyroidism among infertile women in Finland. Gynecol Endocrinol. 2000 Apr;14(2):127-31. doi: 10.3109/09513590009167671. PMID: 10836200.
[2] Busnelli A, Paffoni A, Fedele L, Somigliana E. The impact of thyroid autoimmunity on IVF/ICSI outcome: a systematic review and meta-analysis. Hum Reprod Update. 2016 [3] Nov;22(6):775-790. doi: 10.1093/humupd/dmw019. Epub 2016 Jun 20. Erratum in: Hum Reprod Update. 2016 Nov;22(6):793-794. doi: 10.1093/humupd/dmw034. PMID: 27323769.
[4] Poppe K, Velkeniers B, Glinoer D. Thyroid disease and female reproduction. Clin Endocrinol (Oxf). 2007 Mar;66(3):309-21. doi: 10.1111/j.1365-2265.2007.02752.x. PMID: 17302862.
[5]Jølving LR, Nielsen J, Kesmodel US, Nielsen RG, Nørgård BM, Beck-Nielsen SS. Chronic diseases in the children of women with maternal thyroid dysfunction: a nationwide cohort study. Clin Epidemiol. 2018 Sep 28;10:1381-1390. doi: 10.2147/CLEP.S167128. PMID: 30310330; PMCID: PMC6167124.
